
You're Having a Baby! Vaginal Delivery or Scheduled C-Section??
Pregnancy, labor, and childbirth can be exciting, nerve-wracking, and unpredictable. Vaginal delivery is the most common type of delivery, but about one third of deliveries happen via cesarean section. The majority of c-sections are done due to medical indications (breech presentation, repeat c-section, twins, etc).
A cesarean delivery on maternal request means that a patient requests a c-section and this is done based on her request rather than a maternal or fetal indication. There are risks and benefits of this type of planned c-section just as there are risks and benefits of a planned vaginal delivery. Research on this subject is somewhat limited, and there is no definitive guideline that physicians follow when planning delivery. It is important for physicians and patients to discuss the pros and cons and individualize the treatment plan for each patient. A c-section on maternal request is generally not recommended, but can be performed for the right patient after appropriate counseling.

Image Credit: www.shutterstock.com
When counseling a patient about a c-section, it is important to consider her specific medical problems and risk factors. These include her age, weight, medical problems, past surgeries, future family plan, her personal values and her cultural context. Patients should be educated about labor and delivery, and childbirth, so that misconceptions and fears are not the reason for c-section request. Medical risks and benefits should be considered as well as patient preference. Women may have different reasons to request a c-section. Below I have summarized the common pros and cons expressed by patients and also medical research.
Pros of Planned Vaginal Delivery and C-Section

Cons of Planned Vaginal Delivery and C-Section
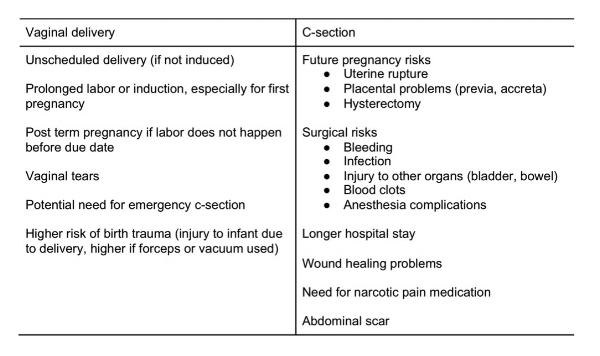
Below is a more detailed summary of the medical risks and benefits, for both the mother and the infant.
Maternal Outcomes
A planned vaginal delivery requires a shorter hospital stay, has a lower risk of infection, fewer complications of anesthesia, and higher breastfeeding initiation rates. However, after 3 and 24 months, breastfeeding rates are similar for vaginal deliveries and c-sections.
A planned c-section has a lower risk of postpartum hemorrhage and transfusion (though the average blood loss in a c-section is greater than in a vaginal delivery). There is a decrease in urinary incontinence during the first year, but after 2 and 5 years, there is no difference in urinary incontinence when comparing women who have vaginal deliveries and c-sections.
There is not a significant difference in postpartum depression, sexual function, and risk of death when comparing vaginal deliveries and c-sections.
Risks of a planned c-section include greater complications in subsequent pregnancies. This is because the scar on the uterus has a very small chance of rupture, and can also cause problems with placental implantation. Problems with the placenta include placenta previa (where the placenta is low and covering the cervix) and placenta accreta (where the placenta has invaded the muscle of the uterus and does not separate after delivery).
These placental complications can sometimes cause life-threatening bleeding and require a patient to need a hysterectomy directly following the cesarean delivery. A cesarean hysterectomy can be a complicated surgery that may require blood transfusion and intensive care stay. The risk of hysterectomy increases as the number of repeat c-sections increases. It is important to consider planned family size when planning mode of delivery.
Infant Outcomes
Elective c-section should only be done after 39 weeks because there is an increased risk of breathing problems, difficulty regulating temperature, and low blood sugar when comparing c-sections and vaginal delivery at less than 39 weeks.
The potential benefits of planned c-section include lower fetal mortality, lower infection rate, lower intracranial hemorrhage, and fewer birth injuries. C-section delivery by 40 weeks could reduce infant mortality because planned vaginal deliveries can occur up to 42 weeks, and the risk of stillbirth increases as pregnancies progress past the due date.
Because there is not great evidence for all the outcomes listed above, the table below summarizes the variables with the strongest evidence, as determined by the NIH State-of-the-Conference Statement on cesarean delivery on maternal request.

Data from NIH State-of-the-Science Conference Statement on cesarean delivery on maternal request. NIH Consens State Sci Statements 2006;23:1–29.
The American Congress of Obstetricians and Gynecologists has the following recommendations:
- In the absence of maternal or fetal indications for cesarean delivery, a plan for vaginal delivery is safe and appropriate and should be recommended.
- The following is recommended in cases in which cesarean delivery on maternal request is planned:
- Cesarean delivery on maternal request should not be performed before a gestational age of 39 weeks.
- Cesarean delivery on maternal request should not be motivated by the unavailability of effective pain management.
- Cesarean delivery on maternal request particularly is not recommended for women desiring several children, given that the risks of placenta previa, placenta accreta, and gravid hysterectomy increase with each cesarean delivery.
If you are thinking about requesting a c-section for delivery, you can see that there are many variables to consider. You should discuss your wishes with your OB/gyn, and make sure that you are aware of the risks of surgery, and specifically the risk for future pregnancies.
References
American Congress of Obstetricians and Gynecologists. Cesarean Delivery on Maternal Request. Committee Opinion 559. April, 2013.

By Loriana Soma, M.D. - Expert OB/GYN