
Depression and Anxiety: Therapy and/or Meds?
Approximately 18.1% of American adults meet criteria for an anxiety disorder and 9.5% meet criteria for a mood disorder in the past year [1].
In an age when 1 in 5 people suffer from clinical levels of depression and anxiety, and many more who are below the threshold, it has become commonplace for people to be taking psychotropic medications or seeing a therapist for these problems. Today’s post will introduce some of the important vocabulary when it comes to treatments that work for depression and anxiety, and the advantages and disadvantages of each approach. Ultimately, clinical decisions are based on a combination of factors, including an informed visit with your doctor.
Who?
Psychotropic medications are prescribed by psychiatrists, who typically hold M.D. degrees after attending medical school and completing a general psychiatry residency program. These medications can also sometimes be prescribed by your family doctor or primary care physician, since many of these doctors are comfortable prescribing them and they are so commonly prescribed. However, these doctors have typically not gone on to receive specialized training in psychiatry.
Therapy, on the other hand, is provided by a broad class of clinicians called psychotherapists. Of these, psychologists hold Ph.D. or Psy.D. degrees after attending graduate school for their doctoral degrees, social workers hold LICSW degrees after obtaining a masters in social work, and mental health counselors hold LMHC degrees. All of these types of therapists require getting licensed by the state in order to begin practicing therapy.
What?
Psychotropic Medications
The most common and empirically-supported psychotropic medications for treating depression and anxiety are a class of drugs known as antidepressants. About 13% of American adults reported taking antidepressants in a major study published in 2015 [2]. Contrary to what the name sounds like, these drugs are also highly efficacious for treating anxiety due to their anxiolytic properties.
Antidepressants can be broken down into more types, which act on different neurotransmitters, such as monoamine oxidase inhibitors (MAOIs), tricyclics, serotonin selective reuptake inhibitors (SSRIs), and serotonin norepinephrine reuptake inhibitors (SNRIs), with the latter two classes being the newest and most commonly prescribed. These include: Prozac, Lexapro, Zoloft, Luvox, Paxil, Cymbalta, and Effexor (all trade names).
Other common drugs prescribed specifically for anxiety are benzodiazepines (such as Valium, Klonopin, Ativan, Xanax- all trade names) and beta-blockers (such as propranolol). Some of the benzodiazepines can have addictive properties, and may reduce the efficacy of cognitive behavioral therapy, when used concurrently, especially when they are taken before or during an exposure exercise.
Therapy
In terms of therapy, the most well-supported psychological treatment for depression and anxiety is cognitive behavioral therapy (CBT), which contains two important elements: cognitive therapy and behavioral therapy (also known as exposure therapy). CBT is a short-term, time-limited, skills-based therapy. There are many clinicians in the community who claim to practice CBT but actually use much more eclectic methods or diluted cognitive or behavioral methods, so it can be very difficult as a patient to determine whether you are actually receiving CBT. For this reason, it is a good idea to ask about their training background.
Some good indicators of CBT include receiving specific between-session homework assignments, in-vivo or imaginal exposure to feared stimuli or situations either during the office visit or outside or both, and recording maladaptive thinking patterns and/or behaviors that maintain the cycle of distress.
When?
Antidepressants have a delayed effect and can take between 2-4 weeks for an adequate trial. For obsessive compulsive disorder and body dysmorphic disorder, higher doses are often needed and for longer durations (up to 14 weeks). These medications must be taken daily.
CBT in general takes between 12-20 sessions, but briefer treatments have been developed and tested. For example, five-session protocols have been developed for depression and panic disorder. Sessions typically last 50-60 minutes, with some sessions lasting longer to accommodate exposure exercises (90 minutes).
When it comes to deciding for yourself or a family member what kind of treatment to pursue, the decision will come down to personal preferences and your doctor’s recommendation. Often the clinical intuition in severe cases is to try a combination of CBT and medications.
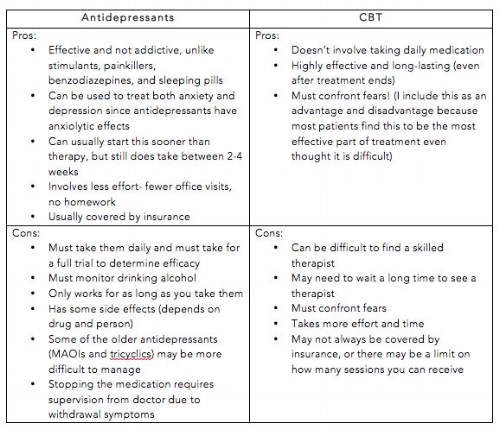
Studies have shown that the effects are comparable between CBT and antidepressants for both depression and anxiety, but in severe cases of depression, cognitive therapy may have longer-lasting effects and reduce the risk of relapse [3]. Similar findings have been reported for anxiety [4]. Below, I have broken down some of the advantages and disadvantages to each approach:
Additional resources and reading on this topic can be found online:
http://www.abct.org/Help/?m=mFindHelp&fa=CBT_Or_Medication
https://adaa.org/about-adaa/press-room/multimedia/treating-anxiety-part3
https://www.nimh.nih.gov/health/topics/index.shtml
References:
1. Kessler, R. C., Chiu, W. T., Demler, O., Merikangas, K. R., & Walters, E. E. (2005). Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry, 62(6), 617-627.
2. Kantor, E. D., Rehmn, C. D., Haas, J. S., Chan, A. T., & Giovannucci, E. L. (2015). Trends in prescription drug use among adults in the United States From 1999-2012. JAMA, 314, 1818-1830.
3. Hollon, S. D., DeRubeis, R. J., Shelton, R. C., Amsterdam, J. D., Salomon, R. M., O'Reardon, J. P.,…Gallop, R. (2005). Prevention of relapse following cognitive therapy vs medications in moderate to severe depression. Arch Gen Psychiatry. 62(4), 417-422.
4. Hollon, S. D., Stewart, M. O., & Strunk, D. (2006). Enduring effects for cognitive behavior therapy in the treatment of depression and anxiety. Annu Rev Psychol, 57, 285-315.

By Angela Fang, Ph.D. - Expert Psychologist